
Citation: Pickhardt PJ, Correale L, Hassan C. CT Colonography versus Multitarget Stool DNA Test for Colorectal Cancer Screening: A Cost-Effectiveness Analysis. Radiology. 2025;315(3):e243775. doi:10.1148/radiol.243775

Lead Author
Dr. Perry J. Pickhardt, MD
Founding Clinical Advisor, ColoWatch® • Professor of Radiology, University of Wisconsin
Dr. Pickhardt is one of the world's foremost authorities on virtual colonoscopy (CT colonography), having authored the landmark 2003 New England Journal of Medicine study that established it as a viable screening tool. His continued research is central to ColoWatch®'s mission of expanding access to safer, more effective colorectal cancer screening.
Key Results
- CRC incidence reduced by 70–75% with virtual colonoscopy (CTC) strategies, compared to only 59% with Cologuard (mt-sDNA testing)
- Virtual colonoscopy (CTC) is cost-saving — it actually costs less than no screening at all, while Cologuard costs $8,878 per quality-adjusted life year gained
- A conventional virtual colonoscopy (CTC) strategy of polypectomy for all polyps measuring at least 6 mm was not cost-effective relative to a surveillance strategy for small (6–9 mm) polyps; the increased costs of colonoscopy did not offset the small gain in QALYs
The Bottom Line: Virtual Colonoscopy Dominates
The results of this study are unequivocal. In a simulated cohort of 10,000 individuals representative of the 45-year-old U.S. population, all three screening strategies were clinically effective compared with no screening — but varied dramatically in both cancer prevention and cost:
In health economics, when a strategy is described as “dominant,” it means it is both more effective and less expensive than the alternatives — the best possible outcome in a cost-effectiveness analysis. Both virtual colonoscopy (CTC) strategies achieved this distinction over Cologuard and no screening.
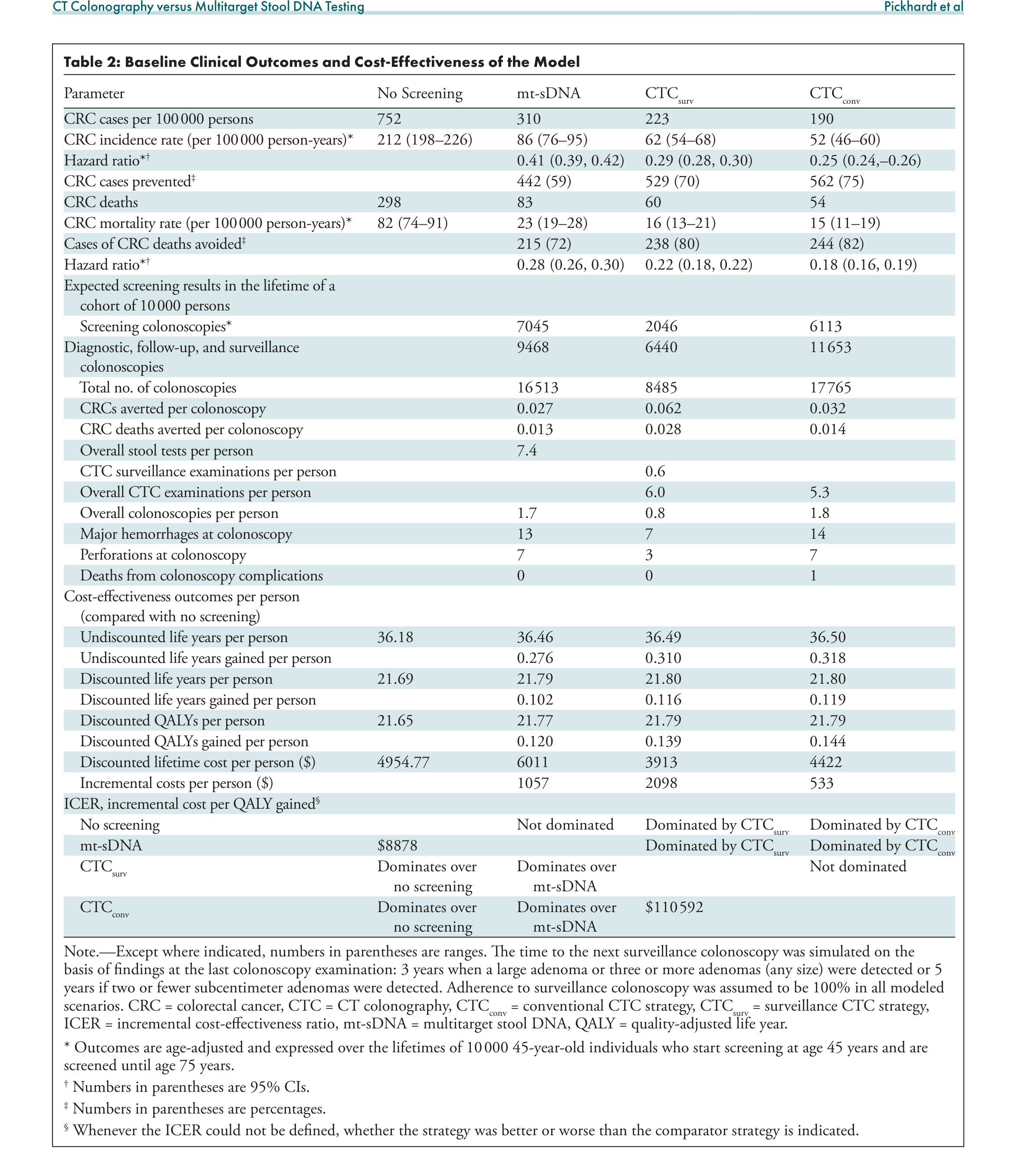
Table 2. Baseline clinical outcomes and cost-effectiveness of the model across all screening strategies. Virtual colonoscopy (CTC) strategies demonstrate lower costs, fewer CRC cases, and fewer deaths compared to mt-sDNA testing.
Why Virtual Colonoscopy Outperforms Cologuard
The study highlights several fundamental differences between these screening modalities:
- Superior polyp detection: Virtual colonoscopy (CTC) detects 85% of large polyps and 70% of small polyps, compared to Cologuard’s 42.4% sensitivity for large polyps and just 17.2% for small/diminutive polyps. Since removing precancerous polyps is the primary mechanism for cancer prevention, virtual colonoscopy’s superior detection translates directly into greater cancer prevention.
- Actionable information: A positive virtual colonoscopy (CTC) provides detailed data on polyp size, number, location, and morphology — enabling tailored clinical management. A positive Cologuard result is binary (positive/negative) with no specific information, and its positive predictive value for actual cancer is only about 2%.
- Fewer unnecessary colonoscopies: Despite being more clinically effective, the virtual colonoscopy (CTC) surveillance strategy results in dramatically fewer total colonoscopies (8,485 vs. 16,513 for mt-sDNA per 10,000 people), reducing procedure-related complications and costs.
- Robust across all scenarios: Even when researchers drastically altered assumptions — reducing Cologuard’s cost by 95% (from $531 to $25) or increasing virtual colonoscopy's (CTC) cost by 250% (from $493 to $1,234) — virtual colonoscopy (CTC) still remained cost-effective.
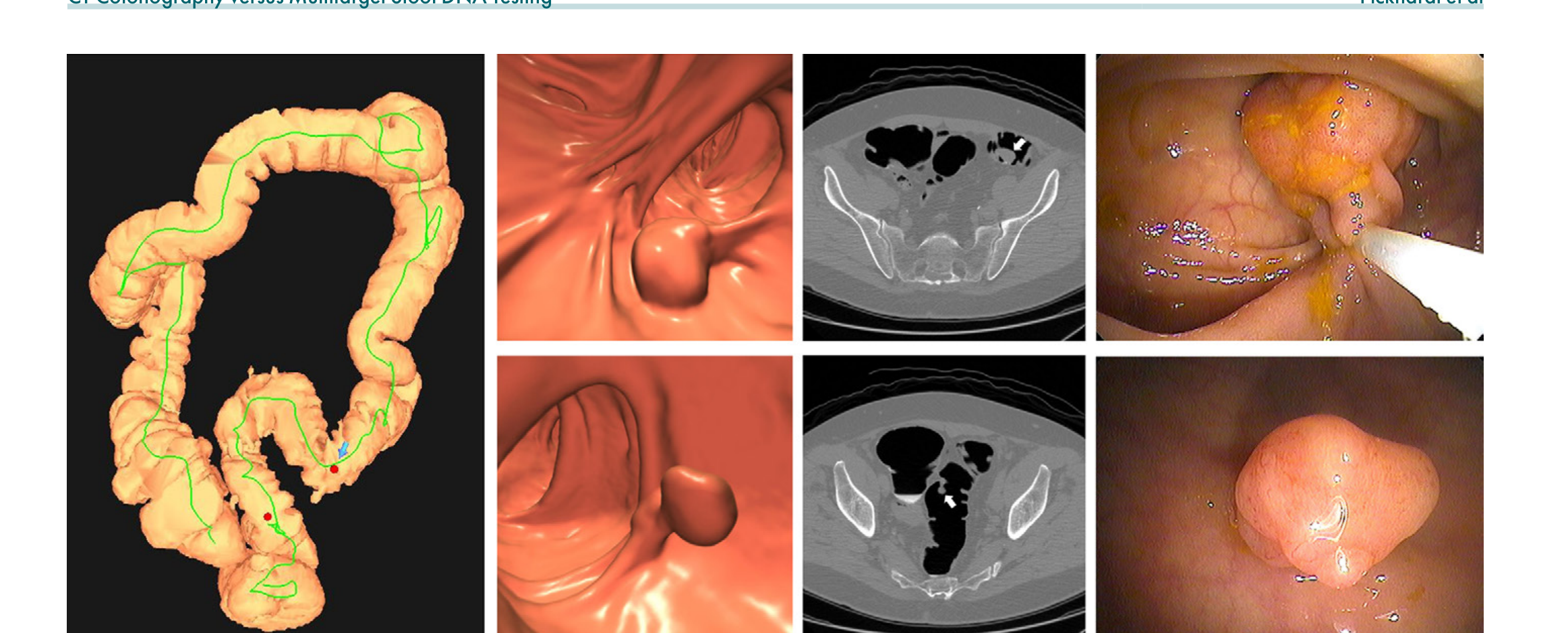
Figure 2. Images from a positive virtual colonoscopy (CTC) screening in an asymptomatic 67-year-old man, showing a large 1.6 cm pedunculated polyp (tubulovillous adenoma) and a 9 mm polyp — both confirmed and resected at same-day optical colonoscopy. Compare this level of actionable information with a positive mt-sDNA test result, which provides no specific details.
The “Goldilocks Zone” of Screening
“CTC screening is ideally positioned in a ‘Goldilocks zone’ that emphasizes cost-effective cancer prevention and early detection.”
— Dr. Perry J. Pickhardt, Radiology, 2025
This philosophy is captured in the virtual colonoscopy (CTC) screening mantra: “Ignoring the tiny, watching the small, and removing the large” — referring to how diminutive (≤5 mm), small (6–9 mm), and large (≥10 mm) colorectal polyps are respectively managed. This approach achieves the ideal balance between cancer prevention and cost-effectiveness.
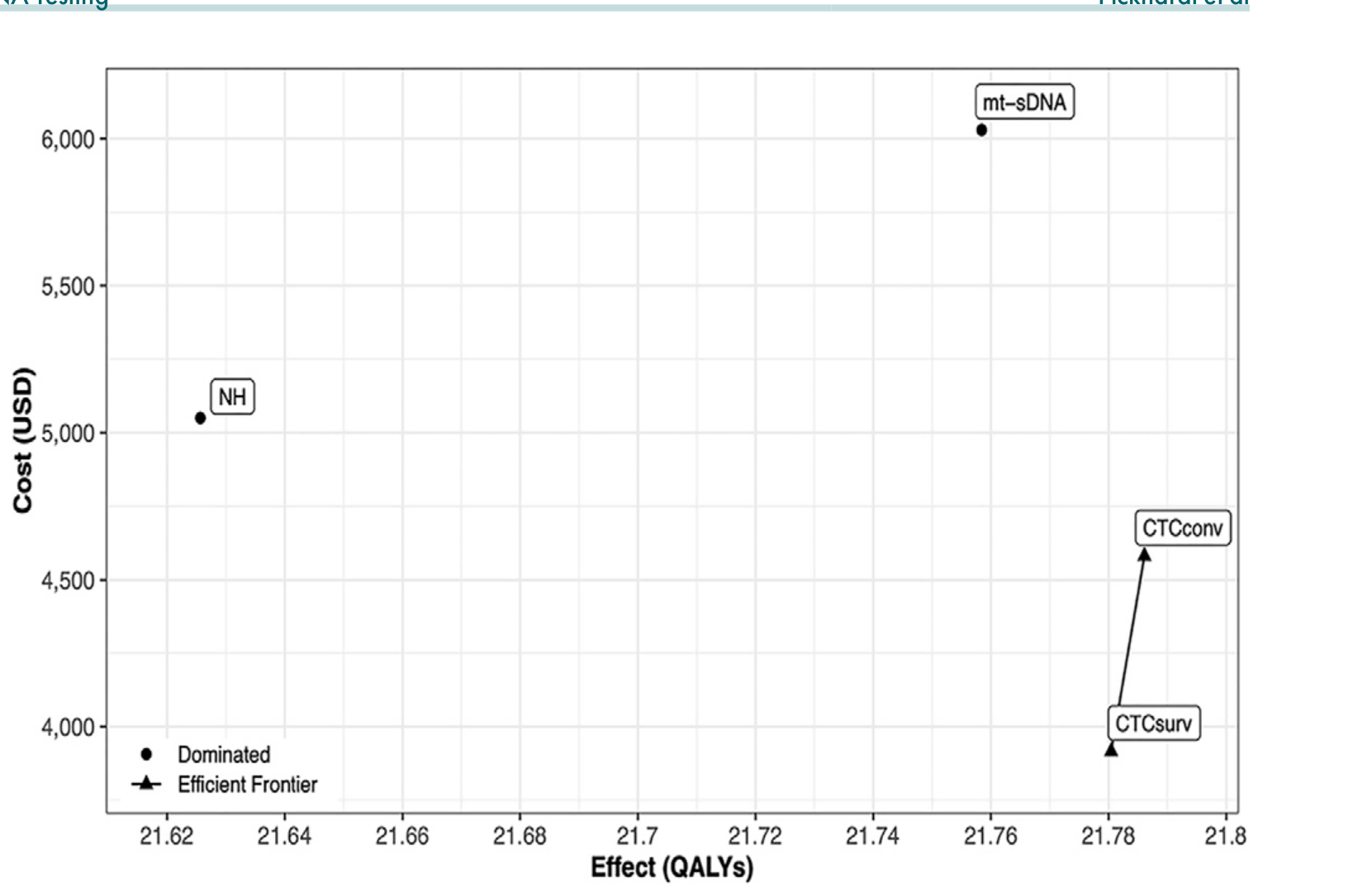
Figure 3. Cost-effectiveness plane showing that both virtual colonoscopy (CTC) screening strategies fall in the dominant quadrant — less costly and more effective — compared to both mt-sDNA testing and no screening. The no screening and triennial mt-sDNA strategies were dominated.
What This Means for Patients
For everyday Americans considering colorectal cancer screening, the implications of this study are profound:
- Virtual colonoscopy prevents more cancer than the heavily-advertised stool DNA test, while costing less overall.
- 90% of patients screened with virtual colonoscopy (CTC) will need no further testing for 5 years — no sedation, no time off work, no ride home needed.
- The 15-minute, noninvasive procedure has zero reported deaths worldwide in over 25 years of use.
- Virtual colonoscopy can also detect unsuspected non-colon cancers and other significant findings — an additional benefit that stool tests — and colonoscopy — cannot provide.
📄 Read the Full Study
This article summarizes the key findings from the original 12-page peer-reviewed publication. For the complete methodology, all tables, supplemental data, and the full list of 49 references, download the original paper.
Download Full Study (PDF)